Say Good Riddance to Vaginal Dryness and Painful Sex
Find out the cause and the most effective things you can do to reverse the problem
Dr. Mache Seibel: At the annual meeting of the North American Menopause Society (NAMS), I interviewed one of the America’s top sex experts Dr. Sheryl Kingsberg on a very common symptom of menopause: vaginal dryness and painful sex.
MS: Can you discuss what is meant by vulvovaginal atrophy?
Dr. Sheryl Kingsberg: Vulvovaginal atrophy is a part of a bigger condition we now call genitourinary syndrome of menopause. It refers to loss of the vaginal and urogenital tissues caused by loss of estrogen at menopause.
MS: Vulvovaginal atrophy sounds awful.
SK: One of the reasons we now call it genitourinary syndrome of menopause is because women do not like to think of themselves as atrophying.
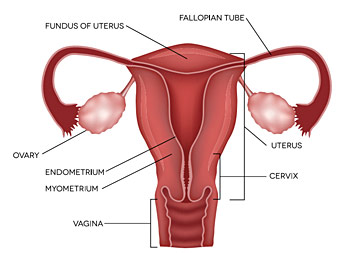
MS: So estrogen goes down and the vaginal tissues get thinner, narrower and shorter.
SK: And drier.
MS: And drier. Which causes?
SK: Which causes pain with sexual activity. It can also interfere with everyday functioning. Exercise can become painful and even getting on the floor with your grandkids can sometimes be a problem.
MS: How common is this?
SK: We have 64 million postmenopausal women in the United States. About half or 32 million of them have symptoms of vulvovaginal atrophy; and only 7% of them are getting prescription therapies.
MS: Why is this so low, why wouldn’t they want something done?
SK: I think there are a few reasons. First of all, women don’t recognize this problem is associated with menopause because it tends to happen a few years later than the beginning of menopause, so they don’t tie it to lower estrogen levels. Also, They don’t realize those symptoms are medical symptoms/conditions so they don’t think to ask their healthcare provider about it, or offer it up if they’re asked about symptoms. In addition, pain with sexual activity or vaginal dryness is a little embarrassing for some women to discuss with their healthcare provider. And healthcare providers often forget to ask their female patients about this. When they do talk about prescription therapies, most of them are local estrogen therapy. So often the word “estrogen” sends women running to the hills for fear of developing breast cancer, which is inaccurate.
MS: So women are afraid or embarrassed to tell, and doctors, either because of time or other reasons don’t ask. That leaves women untreated and basically having to grin and bear something that is really painful, difficult for their relationships and also, I’m sure, bad for self-esteem.
Vulvovaginal atrophy not only doesn’t go away, it gets progressively worse over time if you don’t treat it
SK: Absolutely. In fact, our focus groups showed that beyond painful sexual activity, it causes women to have really impaired self-esteem. They talk about the negative impact it has on their relationships and overall quality of life.
MS: You’ve made a very important point that we kind of glossed over - estrogen. I know that if it has estrogen in it, the law currently requires the manufacturer to place “a black box warning” on it that says the product could cause breast cancer, even if it’s a low dose put locally into the vagina.
SK: I think it does a disservice to women to have that in the package insert, because essentially anything that contains estrogen has the same exact warning label. But local estrogen is not systemically absorbed, or if it is, it is a minute amount. For example, one year’s worth of using Vagifem, which is one of the local estrogen options, gives you the equivalent systemic absorption of one birth control pill; one year, one pill.
MS: So, one year of taking the vaginal estrogen Vagifem increases blood estrogen levels equivalent to taking one birth control pill, one time.
SK: Correct. Which is essentially none.
MS: Do vaginal creams or other vaginal estrogens also cause low levels of absorption?
SK: Yes, they are all very low levels; they are local for a reason. You put them in your vagina and they mostly stay in your vagina and work on the vaginal tissue. The package insert lists the same warnings as somebody taking an oral estrogen that is systemically absorbed, and that causes women a lot of fear with vaginal estrogen. And as we learn more about estrogens, even those given systemically can be safe. Unfortunately, that label really misinforms women about the risk of local estrogen.
MS: Another reason you said women don’t ask for treatment is because they think vaginal dryness or painful sex, like hot flashes, will eventually go away. Is that the case?
32 million women have symptoms of vulvovaginal atrophy; and only 7% of them are getting prescription therapies
SK: Women do assume that, like hot flashes, vulvovaginal atrophy will eventually go away. But the fact is that vulvovaginal atrophy not only doesn’t go away, it gets progressively worse over time if you don’t treat it. If you do treat it, you can probably reverse many of the changes that did happen if you haven’t been treated and it can keep the vagina healthy so you can use it for many years. I really think that women should be talking to their healthcare providers about this.
MS: Do you feel that estrogen locally is by far the best treatment for vulvovaginal atrophy?
SK: It is the most used option of our 7% that are getting treated. There is also an oral non-estrogen medicine called Osphena that has only a local effect and can be used for women who are uncomfortable with vaginal treatments or don’t want to take estrogen. Osphena is a SERM (Selective Estrogen Receptor Modulator) that has been shown to be effective in treating painful sex associated with menopausal changes.
Another option on the horizon is vaginal DHEA, dehydroepiandrostenedione, that hopefully will get FDA approved. It has shown great promise in treating vulvovaginal atrophy. So, we have a lot of options that are safe and effective. Women shouldn’t have to suffer in silence. Don’t think, “It’s a part of aging, I should just learn to live with it.” That’s really the wrong attitude, there’s no reason we shouldn’t live fully thriving lives and that means having a healthy vagina.
Sheryl Kingsberg is a Clinical Psychologist and Professor of Reproductive Biology and Psychiatry at Case Western Reserve University School of Medicine as well as Chief of the Division of Behavioral Medicine in the OB/GYN department at University Hospitals Case Medical Center.
Source: My Menopause™ magazine, No. 31

Dr. Machelle M. Seibel is a leading expert in women's health. He is founder of My Menopause Magazine available in the Apple Newsstand and on Google Play. Get a
FREE Subscription at
www.FreeMenopauseHelp.com.